Change Location
You are about to enter the PAJUNK® GmbH
Medizintechnologie (global) website.
If you are from United States,
visit the U. S. Website:
 pajunkusa.com
pajunkusa.comGlobal Website:pajunk.com
You are about to enter the PAJUNK® GmbH
Medizintechnologie (global) website.
If you are from United States,
visit the U. S. Website:
pajunkusa.com
You are about to enter the PAJUNK® GmbH
Medizintechnologie (global) website.
If you are from United Kingdom, Ireland, Malta or India,
visit the UK Website:
 pajunk.co.uk
pajunk.co.uk


Pajunk has always been close with the major Regional Anaesthesia societies by providing our support through attendance of the bigger and smaller meetings, workshops and trainings on the European level. ESRA has been and is very scientific and now open up more towards the industry with different marketing possibilities. Luckily, the pandemic, which caused almost everything to go virtual, had a major impact on ESRA’s decision to work closer with the industry as well. Already now, Pajunk started the first webinar as an official industry partner of ESRA.
This year we plan a total of six webinars together with ESRA.
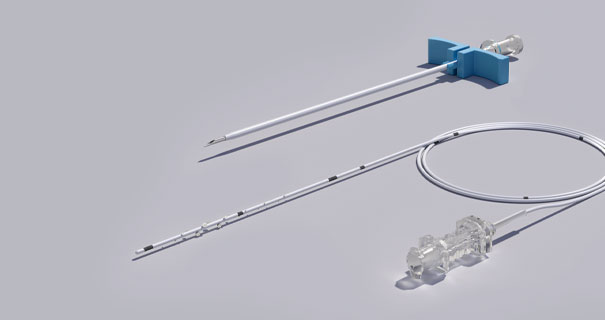
The first webinar took place on Jaunary, 19th and coverd the following topic: Pre-peritoneal wound infiltration catheter in laparoscopic colorectal surgery
The second webinar will take place on February, 18th and will focuse on Ultrasound-guided WALANT & Ultrasound-guided Ophthalmic Blocks. You can register here.
The January webinar Pre-peritoneal wound infiltration catheter in laparoscopic colorectal surgery was led by Dr. F. Jeroen Vogelaar (Surgeon) and Dr. Ansgar Harm (Anesthesiologist), both from the VieCuri Medisch Centrum, Venlo (Netherlands). During the session they discussed important topics of opioid sparing technique in laparoscopic procedures on the example of a colorectal surgery:
You can view the webinar on our youtube channel - link see below.
But alcohol has no place in anesthesia and pain therapy.
You only need one catheter if the midline is crossed, easier to perform, faster.
Preperitoneal is just easier and thus faster to perform, one catheter, 5 minutes, good results.
We had no catheter related infections.
You need a certain volume to achieve results.
No.
We just leave them in.
Until now, if a patient is fit enough to go home on day 2, we remove the catheter. Sending a patient home with a catheter for 1 day is not our plan at this moment.
In a pfannestiel-incision it is quite easy to close the peritoneum, because of a lacking posterior fascia (below the linea arcuata). We closed it also before the catheter-era in this incision, also in favour of a better pneumoperitoneum after extracting the specimen.
Just one in the main incision, we infiltrate the other ports.
The few times we converted to an open procedure we placed the catheter on the closed peritoneum. There was some effect of it, but not that optimal as compared to the pfannenstiel. Therefor a tunnelled positioning (even 2) is necessary in laparotomies, but at this time I am lacking experience with that.
That has been tried but with little success.
No, it's just for the abdominal wall, but visceral pain plays a small roll in laparoscopic surgery.
70h
We don't do have many children, but if you make sure not to exceed the (adjusted to weight) maximum amount’s of LA there should be no problems.
We had no catheter related infections.
The slide wasn't clear. It didn't reduce pain scores over all, only in a subgroup of gynaecological patients and only at 48 h. Gupta et al Acta Ans Scand August 2011 Pages 785-796.
Morphine as necessary, earlier we used PCA, but patients rarely needed much morphine.
It can be used at any incision and with rectus sheath you would need two catheters.
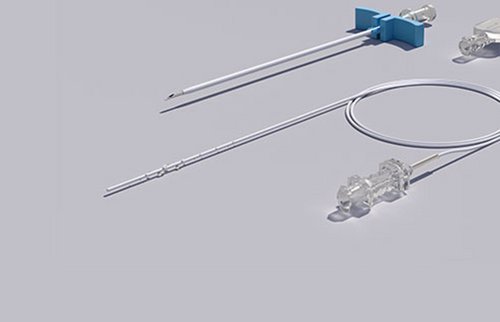
Until the pump is empty, 350ml / 5ml/h = 70 h after start, shorter if we have to use higher volume, with the planned RCT for spondylosis we are planning to use higher volumes and use a second elastomer pump when needed.
Patients are very satisfied during hospital stay. Because it is 'common care' in our hospital, we do not pay a lot of specific attention to this topic after 6 weeks.
In midline incision it is not always easy to place a catheter in the way we do in pfannenstiel incision because the peritoneum if more fixed to the posterior fascia. A tunnel-technique with even 2 catheters seems to be the best way for this, but my experience is lacking at this time. A stoma is not a contradiction itself, but does cause an "integrity-disruption" of the peritoneum which may cause pain itself.
Some colleagues do, the most just use propofol/remifentanyl.
Yes.
In theory it is, I don't have any experience with it. I only use it for rib fractures, VATS and mamma surgery.
We don't use NSAID's not because of possible anastomotic leakage.
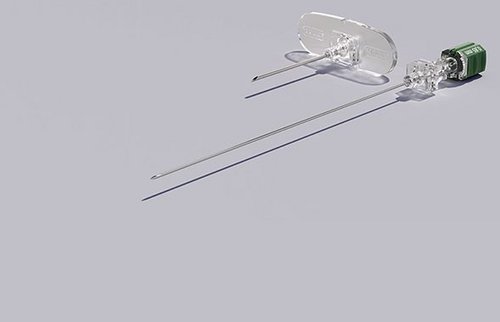
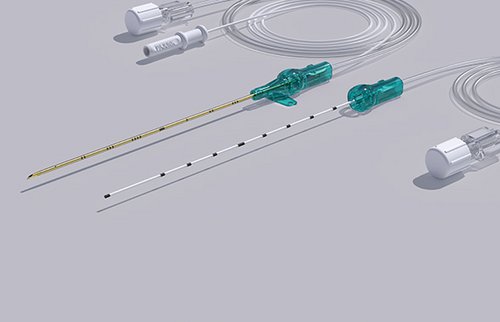
Openings in the catheter over the whole length that is inserted in the wound.
Sure, there are different lengths of catheters and you could also use two short ones.
The length of incision in the pfannenstiel is max 5-7cm. We use the 7cm catheter. For example in C-section I can imagine you use the 15cm.
In general local anaesthetics have an anti-microbial effect (because of the Ph.?). We had no catheter related infectois problems.
Except for abdominoperineal resections there was no difference between colon resections and rectal resections (low anterior). Important difference is of course the perineal wound in APR. A few time we placed also a catheter in this wound with good effect (n=3).
Mean LOS in 2018 in both hospitals was 6 days. With this preliminary results we found a significant reduction to 3-4 days. There will definitely be an ERAS-effect, maybe also any prehabilitation effect, although this was not implemented in the whole study period.
...with reduced opioid and relaxant requirements. But I am looking forward to try this technique as an alternative.
We don't use spinal opioids.
No, only local anesthetics.
Little bleeding, self-terminating, also compressed with closing of wound. You wouldn't insert a catheter if greater bleeding was visible.
There were less ileus than in our historical cohort (epidural).
We had no catheter related infections.
N2O has no place in our hospital for environmental reasons, NSAID's not because of possible anastomotic leakage.
Local anaesthetic at the place of injury.
If it is laparoscopic surgery morphine (PCA or as asked for) With laparotomy we use epidurals.
120 minutes
Intra operative remifentanil, post-operative and as loading dose morphine.
Morphine as necessary, earlier we used PCA, but patients rarely needed much morphine.
Most of the time single shot nerve block, RCT with wound catheters for spondylosis to start soon.
Since we don't use it for caesarean section yet we would look that up in the literature before starting.